This has been quite a stressful week! I’ve had a lot going in the past few days, including moving house, interviews and examinations (so I’ve been kept quite busy!). Luckily everyone’s been really supportive though and by managing my time well and having a number of late nights I’ve managed to stay on top of everything.
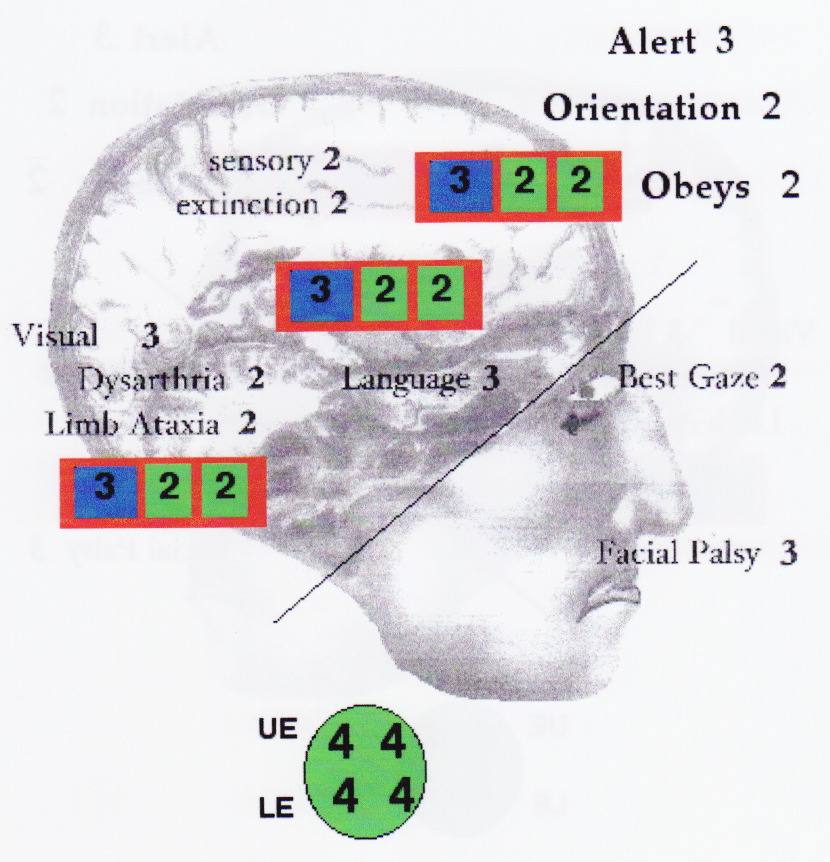
We had a meeting this week to go through the next set of TIA letters for the OSA project. We’re all a lot more in sync now with identifying how patient presentation during TIA events (as described in TIA patient follow-up letters) can be categorised using symptomology-based keywords. For example, someone described as having had a ‘tingling sensation’ would be categorised under paraesthesia and someone described as having been ‘unable to find the correct words ‘ would be categorised under dysphasia. A few examples of these symptoms have been illlustrated below. However, these categories can sometimes be harder to identify from the letters if doctors instead describe the symptoms with broader terms such as ‘sensory’ or ‘speech’ disturbances and sometimes can’t be identified at all if the consultant only talks about their clinic meeting rather than how the TIA originally presented. Having this meeting was really helpful in allowing us to clarify any queries that we had regarding both TIA symptom categorisation, as well as which medications are typically prescribed for hypertension. We are now going to each individually work on categorising these patient letters, with our supervisor uploading new ones as often as possible for us to get on with.
In regards to the SUTO project, this week we were also looking at the patients who had either had a SUTO or undergone a CT perfusion scan between 2010 and 2014, as identified last week. We have now filled in as much of these patients’ information as we can (such as CT results and risk factors) using only the online patient databases. Hopefully this will give us a much clearer template of what remainding patient information we need to look for when going through their paper patient files and will speed things up a bit. However, we still have a huge backlog of patient files that require booking out and are thus limited with the amount of new ones that we can continue requesting before we completely run out of space to store them all! We are hoping to get permission to begin physically collecting and returning patient files from the patient record offices within the next few days, as its starting to limit the project’s progress (and get a bit annoying!). Once this is done though there’ll be no stopping us!
Image retrieved from: http://www.patient.co.uk/health/stroke-leaflet