
Evidence-based medicine has transformed the way in which statistical evidence is used in medicine. Professor Jon Williamson and Dr Michael Wilde, from the Department of Philosophy at Kent, have been working with organisations such as the International Agency for Research on Cancer (IARC) and the UK National Institute of Health and Care Excellence (NICE) to develop better methods for evaluating effectiveness. This has led to a new approach to medicine, called EBM+.
Causal claims are crucial in medicine. Bugs, injuries and environmental factors cause disease and a wide range of harms; medicines, other treatments and public health policies alleviate or prevent such problems. Evidence-based medicine (EBM) offers procedures for assessing the quality of studies that test whether a proposed health intervention is effective. For example, it is common in EBM to grade each study according to how well it was carried out and where it features in a hierarchy of evidence.
In a hierarchy of evidence, studies higher up in the hierarchy are judged to be of higher quality than those lower down. Hierarchies of evidence tend to resemble the hierarchy illustrated in the chart below, which is part of a tutorial on EBM.
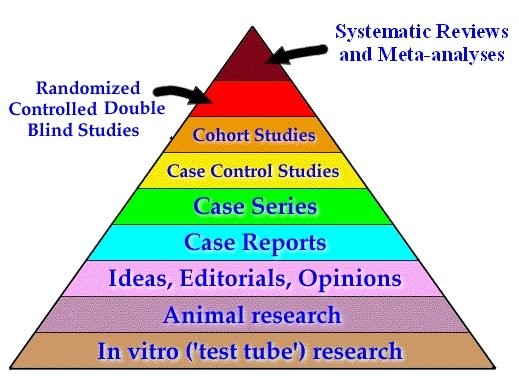
Philosophers have long been interested in whether these judgements of relative quality are justified. While some have questioned whether studies at the top of the hierarchy – systematic reviews, meta-analyses and randomised studies – are as good as they’re made out to be, researchers in the Department of Philosophy have been scrutinising the lower end of the hierarchy.
Jon Williamson, Michael Wilde and colleagues have argued that mechanistic studies (including test tube research) should be treated on a par with the studies higher up the hierarchy, rather than as inferior to them.
Jon Williamson says, ‘Studies higher up the evidence hierarchy sample individuals to see whether more of them had a positive health outcome in the presence of the intervention than in its absence. If such an association is found in the sample, this association could be due to the intervention being effective. Alternatively, it could be due to bias in the way the sampling was conducted, or it could be attributable to some other factor that wasn’t measured. So associations in samples rarely provide conclusive evidence of effectiveness on their own. Evidence of a mechanism linking the intervention and the health outcome can provide further evidence of the effectiveness of an intervention. By appealing to both evidence of associations and evidence of mechanisms, we can reach more conclusive evaluations of effectiveness.’
The EBM+ team argue that evidence of mechanisms should be assessed alongside statistical evidence in order to evaluate whether treatments or health policies are effective. This research could lead to better judgements about which treatments are beneficial, and improved patient outcomes.
This cutting-edge philosophical research is incorporated into undergraduate teaching in the Department of Philosophy, with modules looking at evidence and its evaluation and the philosophy of medicine.
Find out more about EBM+ from the handbook, Evaluating evidence of mechanisms in medicine, or the EBM+ website.